What Is Diabetes Burnout? Signs, Causes, and How to Cope
By Kulmeet Kundlas MD, Board-Certified Internal Medicine — Shield Medical Group, Sebring and Lake Wales, Florida
Have you ever looked at your blood sugar number and just felt like giving up? Not because you’re lazy. Not because you don’t care. But because you are exhausted — mentally, emotionally, physically — from a disease that never takes a day off.
You are not alone. A 2024 International Diabetes Federation (IDF) survey found that 79 percent of people living with diabetes have experienced burnout. And three out of four of those people admitted to stopping or interrupting their treatment because of it.
That’s not a willpower problem. That’s a healthcare crisis hiding in plain sight. Understanding the real diabetes burnout symptoms helps you catch it before it derails your care.
In this guide, I’ll walk you through exactly what diabetes burnout is, how it’s different from depression, why your doctor might be missing it, and most importantly — a clear, step-by-step plan to start feeling like yourself again. Recognizing diabetes burnout symptoms early is the first step toward getting your energy and motivation back.
Watch Dr. Kundlas explain diabetes burnout symptoms, the three-condition frame, and an evidence-based coping plan in this comprehensive video guide.
This post is for you if you have Type 1 or Type 2 diabetes and you’re feeling the weight of it. It’s for you if you love someone with diabetes and want to understand what they’re going through. And it’s for you if you’re a caregiver watching someone you care about slowly pull away from their own health.
Disclaimer: This content is for educational purposes only and is not a substitute for personalized medical advice. Always consult your own healthcare provider for diagnosis and treatment.
The Basics — What Diabetes Burnout Actually Is
Here’s a definition you’ll actually remember: diabetes burnout is what happens when your body and your mind run out of fuel — not from the disease itself, but from the relentless, twenty-four-seven job of managing it.
Imagine you have a second job that you never applied for, that you can’t quit, that doesn’t pay you, that follows you to bed, follows you on vacation, and follows you to every meal. And the only reward for doing it well? Nothing bad happens.
That’s diabetes management. And diabetes burnout is what happens when you can’t do that second job anymore.
The Hidden Cognitive Load
Research shows that people living with diabetes make an estimated 180 extra health-related decisions every single day — over 65,000 additional decisions per year. When to check your sugar. What to eat. How much insulin. Should I exercise now or later. Why is my number high when I did everything right?
That’s not just a lifestyle. That’s a cognitive marathon with no finish line.
Common Diabetes Burnout Symptoms
So what does burnout actually feel like? You might experience:
- Complete exhaustion — not just tired, but empty
- Anger and resentment that diabetes controls your life
- All-or-nothing thinking — “What’s the point? No matter what I do, my numbers are still bad.”
- Skipping blood sugar checks or guessing on insulin doses
- Canceling doctor’s appointments
- Eating whatever you want because you just don’t care anymore
- Social withdrawal — pulling away from friends and family
And here’s what I really need you to understand: this is incredibly common. Over 50 percent of adults with diabetes in the United States experience some level of diabetes distress. For Type 1 diabetes specifically, the prevalence of elevated distress is around 42 percent.
So if you’re reading this and thinking, “That’s me” — you are in the majority, not the minority.
Diabetes Distress vs. Depression
A lot of people — including some doctors — assume that if you’re struggling emotionally with diabetes, you must be depressed. But diabetes distress and clinical depression are not the same thing. Confusing them leads to the wrong treatment. I’ll break down that critical difference in detail below.
If you’re concerned about how stress is affecting your overall health, consider scheduling a comprehensive evaluation at Shield Medical Group to discuss both your physical and emotional well-being.
Why It Matters — The Real Cost of Ignoring This
Let me paint a picture of what diabetes burnout does to your actual life — because the damage goes far beyond blood sugar numbers.
When you’re burned out, everything gets harder. You wake up exhausted. You dread meals because every bite feels like a math problem. You avoid social events because you don’t want anyone asking about your diet. Work suffers because your brain is foggy from the constant mental load. Your sleep suffers. And your relationships take a hit because you don’t have anything left to give.
What Happens Inside Your Body
Chronic emotional stress — the kind that comes from managing a relentless disease — activates your HPA axis, your body’s stress response system. When it stays activated for months or years, it keeps cortisol levels elevated. Cortisol directly raises blood sugar, disrupts sleep, impairs memory and concentration, and drives inflammation throughout your body.
People with diabetes have 4.7 times higher odds of experiencing elevated allostatic load — the scientific term for the total biological wear-and-tear of chronic stress.
The Domino Effect on Blood Sugar Control
The research paints a stark picture of the effects of stress on diabetes control:
- Every 1-point increase on the Diabetes Distress Scale directly increases A1C by 0.41 percent, and drives another 0.24 percent increase indirectly through reduced medication adherence.
- Only 46 percent of patients with clinically significant distress maintain satisfactory medication adherence.
- 33 percent of insulin-treated patients admit to skipping or missing doses at least one day per month.
- Patients with comorbid depression tend to have A1C levels 2 to 3 percentage points higher than those without.
- Poor emotional regulation alone accounts for 42 percent of all effects on a patient’s A1C.
Let me say that differently: how you feel emotionally accounts for nearly half of your blood sugar control. That’s not a side issue. That is the issue.
The financial cost is staggering, too. The annual medical cost of diabetes in the U.S. was over $312 billion in 2015 and is projected to reach $472 billion by 2030. Right here in Florida, the adult diabetes diagnosis rate is 13.1 percent — higher than the national average.
But here’s what I want you to hear: this is manageable. You are not broken. Your pancreas might be. But you are not.
The emotional weight you’ve been carrying? There’s a name for it. There are tools for it. And there is a path forward. Understanding the effects of stress on diabetes control is the first step toward reclaiming your health.
How Doctors Evaluate It — The Three-Condition Frame
Here’s where a lot of people — and honestly, a lot of healthcare systems — get this wrong.
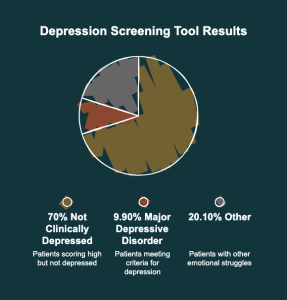
When you tell your doctor you’re struggling emotionally, you might get handed an antidepressant prescription. But research shows that in one study, 70 percent of patients who scored high on a depression screening tool were found not to be clinically depressed when properly evaluated. Only 9.9 percent actually met the criteria for major depressive disorder.
That’s a massive misdiagnosis problem. And it matters because the treatment for diabetes distress and the treatment for clinical depression are completely different.
The Three Conditions Explained
1. Diabetes Distress — The emotional burden that comes specifically from managing the disease. The fear, the frustration, the worry about complications. You’re still engaged in your care, but you’re struggling. You might say things like, “This is so hard,” or “I feel like I’m failing.”
2. Diabetes Burnout — What happens when distress goes unaddressed for too long. You’re not just struggling — you’ve shut down. You’ve stopped checking. Stopped caring. You might say, “I don’t care anymore. What’s the use?”
3. Clinical Depression — A generalized mood disorder. It’s not specific to diabetes. It affects everything in your life. You might say, “I feel hopeless about everything.”
Only about 23 percent of people with diabetes distress also have clinical depression. They can overlap, but they are not the same.
Validated Screening Tools
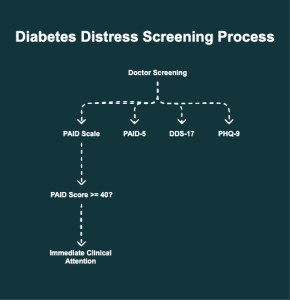
Your doctor can screen for this using validated clinical instruments:
- PAID Scale (Problem Areas in Diabetes) — A 20-item questionnaire that takes about five minutes. A score of 40 or higher means your distress needs immediate clinical attention. There’s a 5-question short form (PAID-5) that is 94 percent sensitive.
- DDS-17 (Diabetes Distress Scale) — Measures distress across four areas: emotional burden, physician-related distress, regimen-related distress, and interpersonal distress.
- PHQ-9 — Screens specifically for clinical depression.
Your takeaway: At your next visit, ask your doctor to screen you for diabetes distress — not just depression. It’s free. It takes five minutes. And it could completely change the direction of your care.
What Actually Helps — Your Coping Plan
This is the most important section. Everything above was building to this moment.
And I want to start with a philosophy I use with my own patients: the goal is not perfection. The goal is sustainability. The opposite of burnout is not trying harder. It’s giving yourself permission to aim for good enough instead of perfect.
Tier 1: Lifestyle and Daily Coping
Stanford Medicine developed a framework called the Four R’s, and it’s one of the most practical strategies available:
- Rest: If you’re not sleeping six to eight hours a night, your blood sugar control will suffer. Sleep deprivation is directly linked to both burnout and poor glycemic control. This isn’t optional — this is medicine.
- Recreation: When was the last time you did something purely for fun? If you can’t remember, that’s a red flag. Schedule it like a doctor’s appointment — because it is one.
- Regular Exercise: Start with the 15-second rule. If you want to exercise but feel overwhelmed, move for literally 15 seconds. Walk. Stretch. Dance. Then take a break. Over two weeks, those intervals naturally build into minutes. Exercise independently reduces diabetes distress and stabilizes blood sugar.
- Relationships: People with diabetes who have strong social support do measurably better. Peer support groups alone produce a pooled A1C reduction of 0.28 percent. Combined with education, that increases to 0.41 percent. That’s the effect of a medication — from human connection.
Another strategy that surprises my patients is the safe diabetes vacation. This is a planned, time-limited, safe break from strict management. Maybe it’s Friday evening — you eat pizza with your family, enjoy dessert, and don’t beat yourself up when your sugar runs a little high. You still take your medications and watch your intake earlier in the day, but you give yourself that mental reset.
One high blood sugar from a planned treat will not doom your long-term health. But chronic emotional exhaustion absolutely will.
Tier 2: Medical and Psychological Interventions
Cognitive Behavioral Therapy (CBT) is one of the most powerful tools available. It teaches you to catch the all-or-nothing thinking that drives burnout — things like “I had one bad number, so I’m a failure” — and replace it with something more accurate: “I’m doing my best with an incredibly hard condition.” Research shows CBT significantly reduces distress, depression, anxiety, and even lowers A1C.
Acceptance and Commitment Therapy (ACT) takes a different approach. It doesn’t ask you to love having diabetes. It asks you to clarify what matters most in your life and take steps toward those values with diabetes in tow. A 2024 meta-analysis found ACT reduced A1C by nearly one full percentage point in people with Type 2 diabetes.
A critical point: Antidepressants generally do not work for diabetes distress. If you are distressed because managing diabetes is exhausting and overwhelming, a pill won’t fix that. What will fix it is adjusting your regimen, getting behavioral support, and having a care team that actually listens. However, if you meet the criteria for major depressive disorder, antidepressants are absolutely appropriate — which is why accurate screening matters so much.
Tier 3: Advanced Support
- Diabetes Self-Management Education and Support (DSMES) can reduce your A1C by 0.6 to 1 full percent — comparable to adding an entirely new medication. Yet fewer than 5 percent of Medicare beneficiaries use it.
- Continuous Glucose Monitors (CGMs) can increase your time in range by 15 to 34 percent and dramatically reduce fingersticks, cutting down on decision fatigue.
If you’re interested in exploring whether DSMES, CGM technology, or behavioral therapy might be right for you, talk to your diabetes care team at Shield Medical Group.
Five Questions for Your Next Doctor Visit
Bring these questions to your next appointment:
- Can you screen me for diabetes distress using the PAID scale or DDS?
- Am I a candidate for CBT or ACT for my diabetes management?
- Are there ways to simplify my regimen to reduce my daily burden?
- Can you refer me to a diabetes educator or DSMES program?
- Am I experiencing distress, burnout, or depression — and how can we tell the difference?
Those five questions could be the turning point in your care.

What Improvement Looks Like
I don’t want to give you false promises. Recovery from diabetes burnout doesn’t happen overnight. But it does happen. Here’s a realistic timeline:
- Within 2 weeks of starting small changes — like the 15-second exercise rule or scheduling one recreational activity — most patients report feeling a slight lift. Not a transformation. A lift.
- At 1 month, if you’ve started working with a therapist or joined a peer support group, you’ll likely notice you’re engaging with your care again. Checking blood sugar more consistently. Not dreading meals as much.
- At 3 months, measurable changes in A1C typically appear. Your A1C reflects three months of blood sugar, so the work you do now shows up on your next lab.
- At 6 months, patients who stick with a combination approach — lifestyle changes, psychological support, and regimen simplification — often describe a genuine shift in how they relate to their disease.
- At 1 year, the identity shift happens. You stop being “the person who is losing to diabetes” and start being “the person who manages a hard disease and has a full life.”
In my clinic, what I celebrate with my patients isn’t a perfect A1C. It’s the moment they walk in and say, “Doc, I checked my sugar every day this week — and I didn’t hate doing it.” That’s a win.
There will be plateaus. There will be setbacks. A bad week doesn’t erase a good month. Progress, not perfection.
Risks, Red Flags, and Mistakes
Let’s talk about the things that can make burnout worse — and the warning signs that mean you need help now.
Seek Help Immediately If…
If you are having thoughts of self-harm or suicide, please call 988 — the Suicide and Crisis Lifeline — or go to your nearest emergency room. Diabetes distress can become that severe, and there is no shame in asking for help.
If you’ve stopped taking insulin or critical medications for more than a few days, that’s a medical emergency — not a willpower failure. Call your doctor today.
Top 5 Patient Mistakes
- Stopping medications cold turkey without telling your doctor. Your body needs that support, even when your mind needs a break.
- Assuming it’s depression and accepting an antidepressant without being properly screened. Remember — 70 percent of those who score high on depression tools actually have distress, not depression.
- Isolating yourself. Research consistently shows that social support is one of the strongest protective factors against burnout.
- Believing social media cure claims. There is no supplement, juice cleanse, or miracle protocol that replaces evidence-based diabetes care. If it sounds too good to be true, it is.
- Waiting too long. Diabetes distress, when left unaddressed, turns into full burnout — and burnout is much harder to climb out of.
A Note for Loved Ones
If you love someone with diabetes — please stop asking them, “Should you be eating that?” That one sentence does more damage than you realize.
The Behavioral Diabetes Institute created a diabetes etiquette card — a free resource available at behavioraldiabetes.org. It teaches friends and family how to actually help instead of becoming the “diabetes police.”
Support means asking, “What do you need from me?” — not policing someone’s plate.
Your Next Steps
Let’s bring this all together with a clear plan:
- Today: Take the free diabetes distress questionnaire at diabetesdistress.org. It’s anonymous, takes five minutes, and tells you exactly where you stand.
- This week: Try the 15-second rule. Pick one form of movement and do it for 15 seconds. Let it count.
- This week: Schedule one recreational activity that has nothing to do with diabetes. Something that’s just for you.
- This month: Bring those five questions to your next doctor’s appointment. Ask to be screened with the PAID scale. Start the conversation about your emotional health — not just your numbers.
- Ongoing: Build your version of the Four R’s — Rest, Recreation, Regular Exercise, Relationships. These aren’t luxuries. They’re medicine.
If you only do one thing after reading this — let it be this: Tell someone how you’re really feeling. Your doctor. Your partner. A friend. A peer group. Break the silence. Because three out of four people who experience burnout stop their treatment. You don’t have to be one of them.
If you’re in the Sebring or Lake Wales area, we’d love to see you at Shield Medical Group. You can reach us through our website or give us a call.
Remember — your pancreas is broken. You are not. Distress is not weakness. Burnout is not failure. They’re signals — and signals can be answered.
This article is for educational purposes only and is not a substitute for personalized medical advice. Always consult your own healthcare provider for diagnosis and treatment.
Frequently Asked Questions About Diabetes Burnout
What is diabetes burnout?
Diabetes burnout is a state of total physical, mental, and emotional exhaustion caused by the relentless daily demands of managing diabetes — not the disease itself. A 2024 IDF survey found that 79 percent of people with diabetes have experienced it, and three out of four of those affected admitted to stopping or interrupting their treatment as a result.
What are the most common diabetes burnout symptoms?
Common symptoms include feeling completely drained, anger or resentment toward the disease, skipping blood sugar checks, guessing on insulin doses, canceling doctor appointments, and withdrawing from friends and family. Over 50 percent of U.S. adults with diabetes experience some level of diabetes distress.
What is the difference between diabetes distress and clinical depression?
Diabetes distress is an emotional response specifically tied to the burden of managing diabetes, while clinical depression is a generalized mood disorder that affects all areas of life. Research shows that only about 23 percent of people with diabetes distress also have clinical depression, and the treatments are different — distress responds to behavioral support and regimen changes, while depression may require antidepressants.
How does stress affect blood sugar control?
Chronic emotional stress activates your HPA axis, keeping cortisol levels elevated, which directly raises blood sugar, disrupts sleep, and drives inflammation. Research shows that poor emotional regulation alone accounts for 42 percent of all effects on a patient’s A1C levels.
What is the PAID scale for diabetes distress?
The PAID (Problem Areas in Diabetes) scale is a free, validated 20-item screening tool that measures the emotional burden of diabetes. A score of 40 or higher on its 0-to-100 scale indicates severe distress needing clinical attention, and a 5-question short form (PAID-5) is available that is 94 percent sensitive.
Can antidepressants help with diabetes burnout?
Antidepressants are generally not effective for diabetes distress or burnout, which are caused by the overwhelming demands of disease management rather than a chemical imbalance. However, if a person meets the clinical criteria for major depressive disorder — which can co-occur with distress — antidepressants are appropriate, making accurate screening essential.
What is the 15-second rule for exercise with diabetes?
The 15-second rule is a habit-building strategy where you start exercising for just 15 seconds at a time — walk, stretch, or dance — then take a break and repeat. Over two weeks, these intervals naturally build into minutes, helping overcome the paralysis of burnout while independently reducing diabetes distress and stabilizing blood sugar.
What are the Four R’s for managing diabetes stress?
The Four R’s is a coping framework from Stanford Medicine: Rest (6-8 hours of sleep nightly), Recreation (scheduled fun activities unrelated to diabetes), Regular Exercise (starting small and building gradually), and Relationships (nurturing social support). Peer support groups alone produce a measurable A1C reduction of 0.28 percent.